Fertility treatments are now widely available and offer both advantages and disadvantages. Researchers are constantly investigating the potential risks associated with these treatments. Some studies suggest that women who become pregnant with the help of assisted reproductive technology may have an increased risk of vascular and pregnancy-related complications.
Fertility Treatments and Cardiovascular Disease
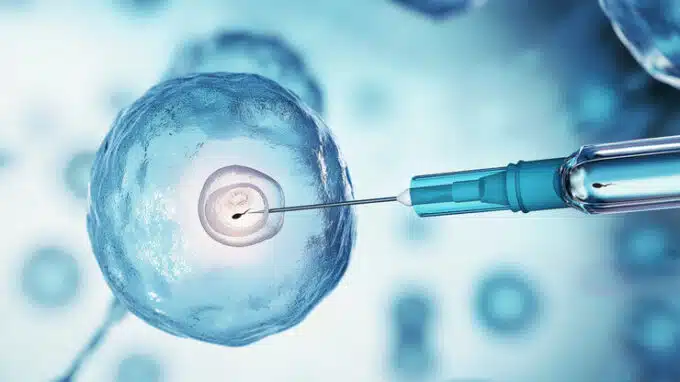
The term assisted reproductive technologies refers to a range of fertility treatments that help increase the chances of pregnancy. These treatments can include the administration of drugs to control ovulation, as well as procedures such as intracytoplasmic sperm injection and in vitro fertilization (IVF), in which eggs and sperm are brought together in a test tube before being implanted into the uterus. According to statistics from the US Centers for Disease Control and Prevention from 2019, the use of assisted reproductive technology has more than doubled in the last ten years.
Older women are increasingly turning to such techniques as the likelihood of pregnancy decreases with age. “However, especially after the age of 35, the risk of developing conditions such as chronic high blood pressure, which increase the risk of pregnancy complications, rises,” said study author Pensée Wu, M.B.Ch.B., M.D., lecturer and honorary consultant obstetrician and sub-specialist in mother and child medicine at Keele University School of Medicine in Staffordshire, UK. “Pregnancy complications such as high blood pressure during pregnancy are now considered risk factors for later cardiovascular disease,” Wu said. According to the researchers, all of this has led to concerns about the negative pregnancy outcomes associated with assisted reproductive technology, but there are few studies on this topic, and their findings are inconsistent.
Analysis Reveals Risks
For this study, the researchers examined data from the U.S. National Inpatient Sample, which includes all hospital discharges between January 1, 2008, and December 31, 2016. They extracted data on all deliveries and, in particular, data that noted the use of assisted reproductive technology and cardiovascular and pregnancy-related complications. The researchers also assessed hospital costs, length of stay, and other factors. The study included more than 106,000 deliveries achieved with assisted reproductive technology and more than 34,167,000 deliveries without ART.

- Women who became pregnant with the help of assisted reproductive technology were older, with an average age of 35, compared to 28 for women who became pregnant without ART.
- Those who became pregnant with the help of assisted reproductive technology also had more pre-existing conditions, such as chronic hypertension, obesity, and diabetes.
- Women who became pregnant through assisted reproductive technology had a more than 2.5 times higher risk of acute kidney damage, also known as acute kidney failure, and they also had a 65% higher risk of arrhythmias (heart rhythm disorders).
- Pregnancy with assisted reproductive technology was associated with a 57% higher likelihood of placental abruption, a serious complication in which the placenta detaches from the uterine lining, as well as a 38% increased risk of cesarean section and a 26% higher risk of preterm birth.
- The increased risks occurred even in women with ART who had no pre-existing cardiovascular risk factors.
- The average hospital costs for women who became pregnant with the help of assisted reproductive technology amounted to US$18,705, compared to US$11,983 for women who became pregnant without ART.
Close Monitoring Important
The study underscores the importance of educating patients considering assisted reproductive technology about health and pregnancy, as well as the risks associated with childbirth. “In particular, patients with existing cardiovascular risk factors should be informed about the potential long-term cardiovascular effects and risks associated with ART, according to the researchers. Women need to know that fertility treatments carry a higher risk of pregnancy complications that require close monitoring, especially during delivery. Primary care physicians and specialists should ensure that these risks are communicated and strategies to mitigate them are discussed and implemented.
A limitation of the study is its retrospective nature, i.e., it is an examination of data collected for reasons other than research, so errors such as misclassification or misdiagnosis may occur. Future research should investigate how optimizing cardiovascular risk prior to assisted reproductive technology affects pregnancy complications and long-term cardiovascular health.
You may also be interested in...
-

If you're a man or woman struggling with infertility, you can take solace in knowing…
-

There is a potential correlation between factors that affect a woman's fertility and her risk…
-
Conditions that affect the heart are broadly called heart disease. Conditions that involve blocked or…


